
It was 2019 when Beth Rempe, then a nurse at Children’s National Hospital in Washington, D.C., first noticed the change.
Doctors were wearing pins sporting the transgender flag. Nurses were asking children, most with no history of gender dysphoria, for their preferred pronouns, which were entered into an electronic record system and documented on white boards outside their rooms. More patients were on puberty blockers and cross-sex hormones, especially young girls. And the top-ranked hospital was telling staff that people could change gender based on their “mood,” according to slides from a mandatory training reviewed by the Washington Free Beacon.
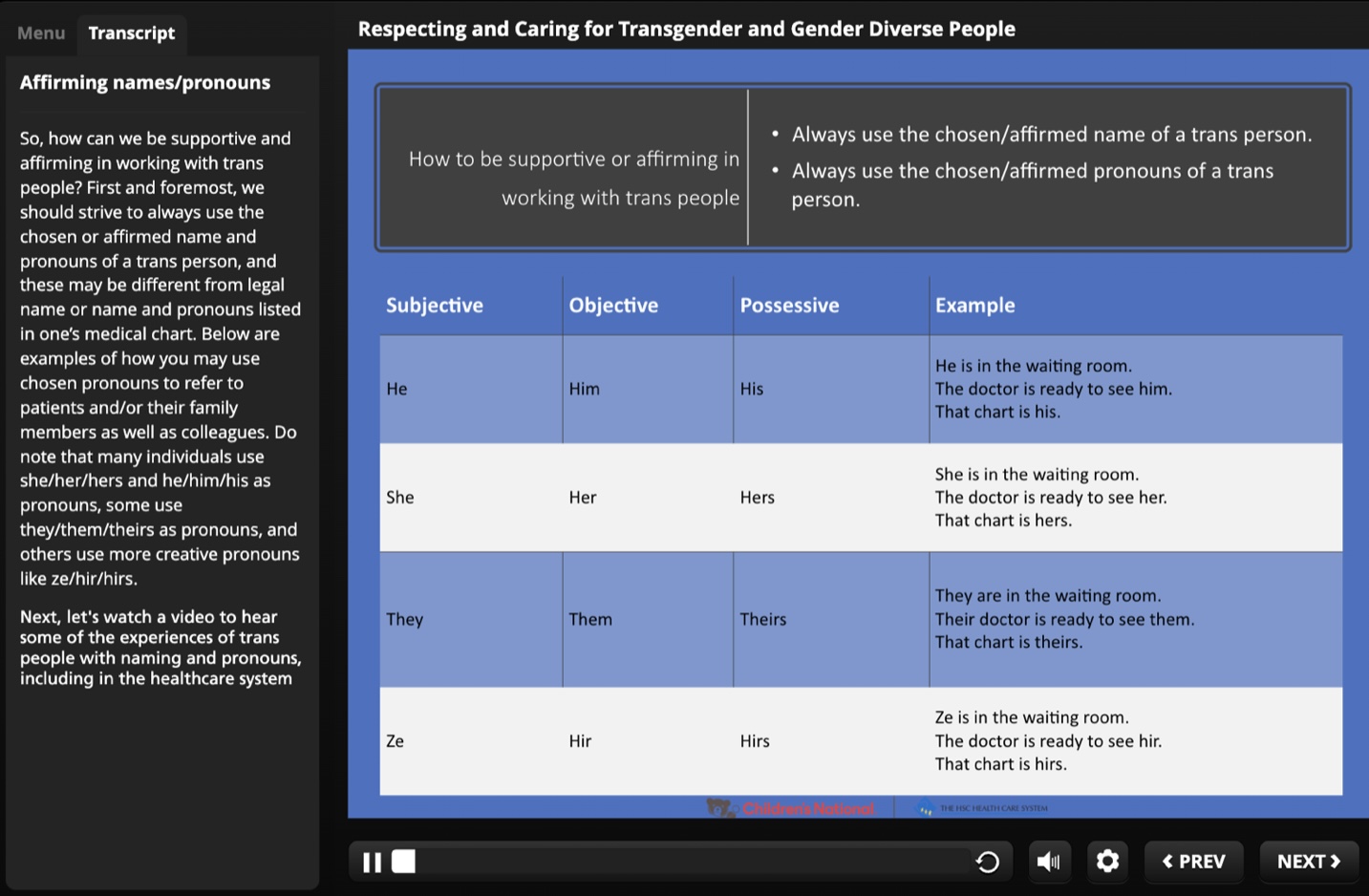
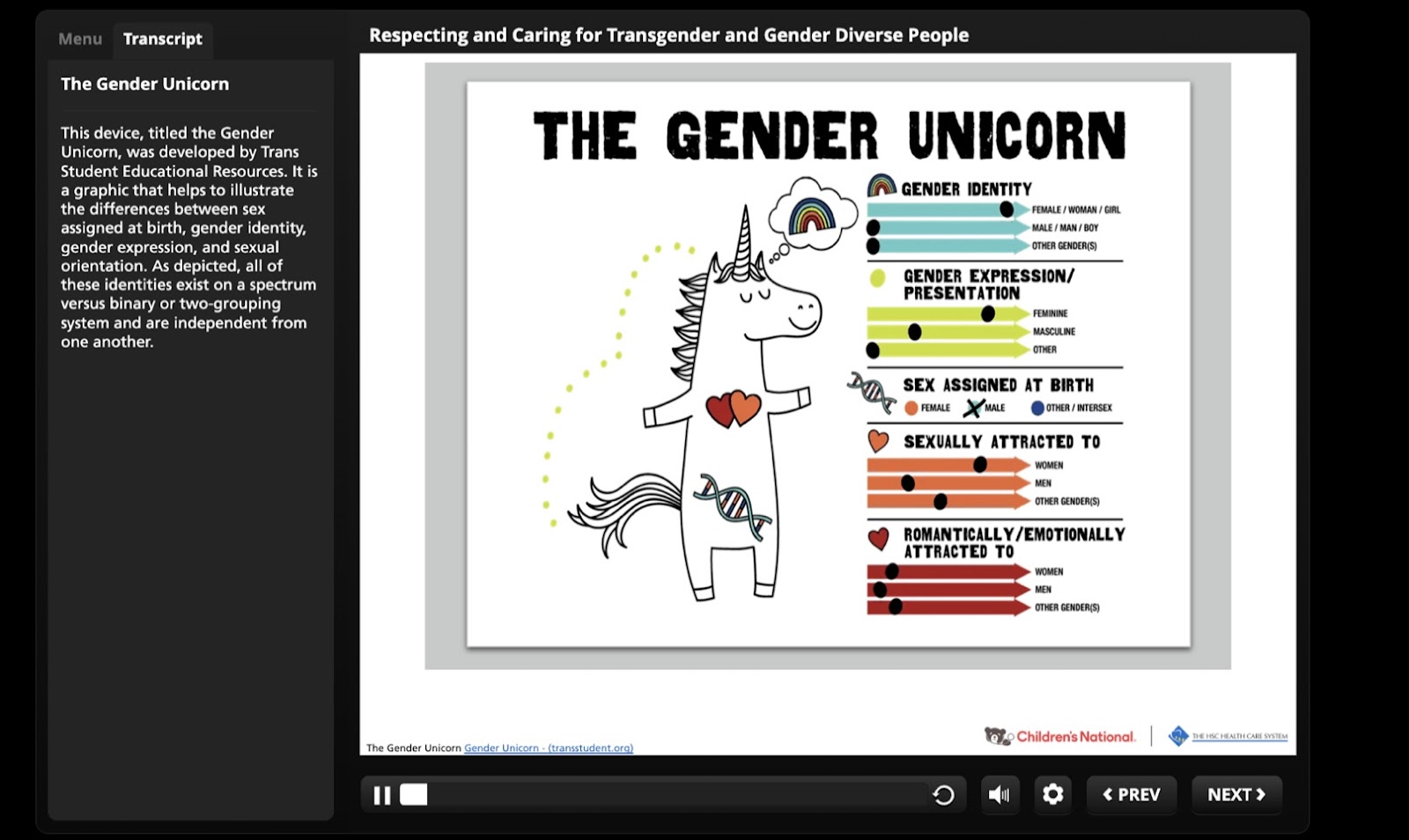
The training, which was offered as recently as January, included a primer on “zi/hir” pronouns and used a “gender unicorn” to illustrate the “spectrum” of “other gender(s).”
By 2022, Rempe said, Children’s National was requiring staffers to use a patient’s preferred pronouns, no questions asked, even as European medical authorities were backing away from that practice, warning that on-demand gender affirmation could entrench dysphoria rather than reduce it, particularly in children. Worried the policy did more harm than good, Rempe asked for an exemption, which the hospital denied. She quit in early 2022.
“I was concerned that I would eventually have to administer puberty blockers and hormones, not just use the pronouns,” Rempe told the Free Beacon. “I kept finding myself in situations I wasn’t comfortable with ethically.”
Since her departure, Rempe has struggled to make sense of what happened to the hospital where she spent 16 years of her professional life. Was there a common thread behind the transgender flag pins, the pronouns, the puberty blockers, and the trainings and policies that enforced the new culture?
As it turns out, there is an outside force pushing hospitals in this direction.
The Human Rights Campaign’s Corporate Equality Index became a flashpoint last month when commentators posited that the scorecard was behind Bud Light’s decision to air an advertisement featuring the transgender TikTok personality Dylan Mulvaney. Well, it has a sibling.
Meet the Healthcare Equality Index, the Human Rights Campaign’s scorecard for hospitals that purports to measure the “equity and inclusion of their LGBTQ+ patients.” The index, which uses a 100 point scale, is funded by Pfizer and PhRMA, the trade association that lobbies on behalf of large pharmaceutical companies. And, Rempe noticed, it awards points for all of the policies Children’s National implemented.
To earn a perfect score, hospitals must display LGBT symbols, solicit and use patients’ preferred pronouns, and conduct trainings on LGBT issues approved by the Human Rights Campaign, according to the scoring criteria. They must also provide the same treatments for gender dysphoria that they provide for other medical conditions—meaning a hospital that uses puberty blockers to treat precocious puberty cannot withhold the drugs from children who say they’re transgender. And though the index does not mention medical conscience exemptions explicitly, it does penalize hospitals for allowing “discriminatory treatment that is in conflict with their non-discrimination policy.”
The Human Rights Campaign is a private entity, and its ratings carry no official weight. But as countries around the world pump the breaks on pediatric transition, critics say that the index—bankrolled by the very companies that produce and profit off puberty blockers and cross-sex hormones—is encouraging the sort of no-guardrails approach that has made U.S. gender medicine an international outlier. The scorecard has helped powerful lobbyists seed their ideology across American hospitals, becoming de facto regulators of health care.
A spokesperson for PhRMA, Brian Newell, downplayed its role in the index, saying the trade association was “not involved in the development” of the scoring criteria. “Our work with the [Human Rights Campaign] has primarily focused on issues impacting patient access and affordability, including for those with HIV,” Newell said.
Pfizer did not respond to a request for comment.
The most coercive part of the index is its “Responsible Citizenship” deduction. Hospitals can lose as many as 25 points for any behavior the Human Rights Campaign deems “discriminatory,” an expansive category that includes statements made by hospital doctors and policies that restrict access to gender medicine, including puberty blockers.
Last year, for example, the Human Rights Campaign deducted points from two Texas hospitals, UT Southwestern Medical Center and Children’s Health in Dallas, because they stopped using puberty blockers to treat gender dysphoria but continued to use them to treat precocious puberty—the blockers’ original purpose.
That “amounts to discrimination against transgender youth,” the Human Rights Campaign argued in a press release.
Another hospital, Mercy San Juan Medical Center in Sacramento, Calif., was docked in 2022 because it refused to perform a hysterectomy on a transgender man, Evan Milton, who was seeking the procedure to eliminate feelings of gender dysphoria. The deduction came on the heels of a lawsuit by the American Civil Liberties Union, which alleged that the Catholic hospital had violated civil rights law by denying the surgery.
Mercy San Juan “withheld medically necessary care for a transgender man while providing the same type of care to cisgender women,” the Human Rights Campaign said in a press release. “Every credible medical organization recognizes the medical necessity of affirming care for transgender and non-binary people.”
Over 2,200 health systems, including dozens of children’s hospitals, have been rated by the index. In 2022, Children’s National earned a perfect score.
This argument—that it is discrimination to provide surgery for one condition and not another—can sound like rhetorical gymnastics. But it has already been accepted by courts and government agencies, which have in some cases forced insurers to pay for sex-change operations.
Citing rules from the Obama administration’s Department of Health and Human Services, for example, a Wisconsin district court ruled that the state’s Medicaid agency had to cover “gender-conforming surgery.” The court’s reasoning was the same as Human Rights Campaign’s: To cover mastectomies for breast cancer but not gender dysphoria, it said, “discriminates on the basis of diagnosis.”
The overlap between legal precedent and the index’s criteria suggest that the latter do have the force of law behind them, in a sense. When the Human Rights Campaign applies the 25 point penalty, it is effectively claiming that a hospital has violated civil rights law. That in turn sends a message to activist groups and the Biden administration, said Rachel Morrison, a former attorney at the Equal Employment Opportunity Commission: “Maybe you should investigate.”
“A bad score puts a target on hospitals’ backs,” Morrison said. “Even if the index itself is not legally enforceable, hospitals still have an incentive to defer to it.”
While the Human Rights Campaign has not sued individual hospitals over their transgender policies, closely-aligned activist groups, including the American Civil Liberties Union and Lambda Legal, have.
“It would be entirely on brand to use the rankings to invite or accelerate lawsuits against hospitals that score poorly,” said Oramel Skinner, Arizona’s former solicitor general who is now the director of the Alliance for Consumers, a nonprofit that defends businesses from class-action lawsuits.
Beyond the veiled legal threat, critics say the scorecard creates reputational incentives to defer to activists instead of medical science, which on transgender issues is increasingly in flux. Hospitals that do well on the index typically incorporate it into their marketing materials, issuing press releases about the quality of their LGBT care.
“My hospital displays a badge on signboards and in emails touting their status as an ‘LGBTQ+ Healthcare Equality Leader’”—the Human Rights Campaign’s designation for hospitals that earn a perfect index score—said a doctor at a large health system in New Jersey, adding that the hospital now requires the front office to ask patients for their preferred pronouns in front of the entire waiting room.
Many health systems seem unwilling to accept anything less than a solid 100. In 2020, after Children’s National only scored a 75, the hospital created a committee focused on boosting its rating, according to a press release. By 2022, it had achieved a perfect score.
Even Johns Hopkins, one of the most prestigious medical centers in the world, appears to have been influenced by the index. In 2018, the Human Rights Campaign docked the hospital 25 points for statements that psychiatrist Paul McHugh, a vocal critic of sex-reassingment surgeries, and another Hopkins doctor, Lawrence Mayer, had made about transgender issues.
Hopkins appears to have opted out of the Healthcare Equality Index annual survey, which gathers information used to complete the scorecard, after incurring that deduction, according to the hospital’s index entry. But by 2022, it had also implemented many of the policies demanded by the Human Rights Campaign, including insurance plans that cover facial reconstructive surgery and data systems that record gender identity and pronouns.
Johns Hopkins did not respond to a request for comment.
The index, which began scoring hospitals in 2017, is far from the only force behind the push for pediatric transition. Plenty of doctors are true believers, Rempe said, and Children’s National was “already motivated” to promote gender medicine before the index came along. Groups like the American Academy of Pediatrics have solidified the consensus, saying that “gender-affirming care” is not only necessary but “lifesaving.”
Though U.S health authorities largely support this treatment model, their European counterparts do not. With rates of transgender identification skyrocketing among young people, especially girls—and amid mounting concerns about the long-term effects of puberty blockers and other treatments—medical bodies across Europe have moved away from the gender-affirming protocols they once championed, imposing new restrictions on pharmaceutical interventions and even urging caution on social affirmation.
Most studies find that gender dysphoria resolves itself by puberty. Social transition, however, has been linked to more persistent feelings of cross-sex identity, suggesting that it could “lock in” the dysphoria it is meant to alleviate, though the reasons for the link remain unproven.
Changing a child’s name and pronouns is “not a neutral act,” a report from the British National Health Service concluded last year. “It is an active intervention” whose long-term effects are unclear.
The Healthcare Equality Index has ignored all these developments. Its scoring criteria, which were updated this year, award points for facilitating both social and physical transition and, aside from a caveat about “intersex children,” includes no guidance on age limits or informed consent.
Points are also awarded for providing “Training in LGBTQ+ Patient-Centered Care” approved by the Human Rights Campaign. Hospitals can either submit their own internal trainings for review or pick from a list of pre-approved modules, which give some idea of what the group is looking for.
One training, offered by Howard Brown Health, teaches participants to “dismantle the gender binary” and “define misgendering as trauma,” according to a description of the training on the Human Rights Campaign’s website, while another discusses “frameworks of care such as intersectionality and anti-oppression.”
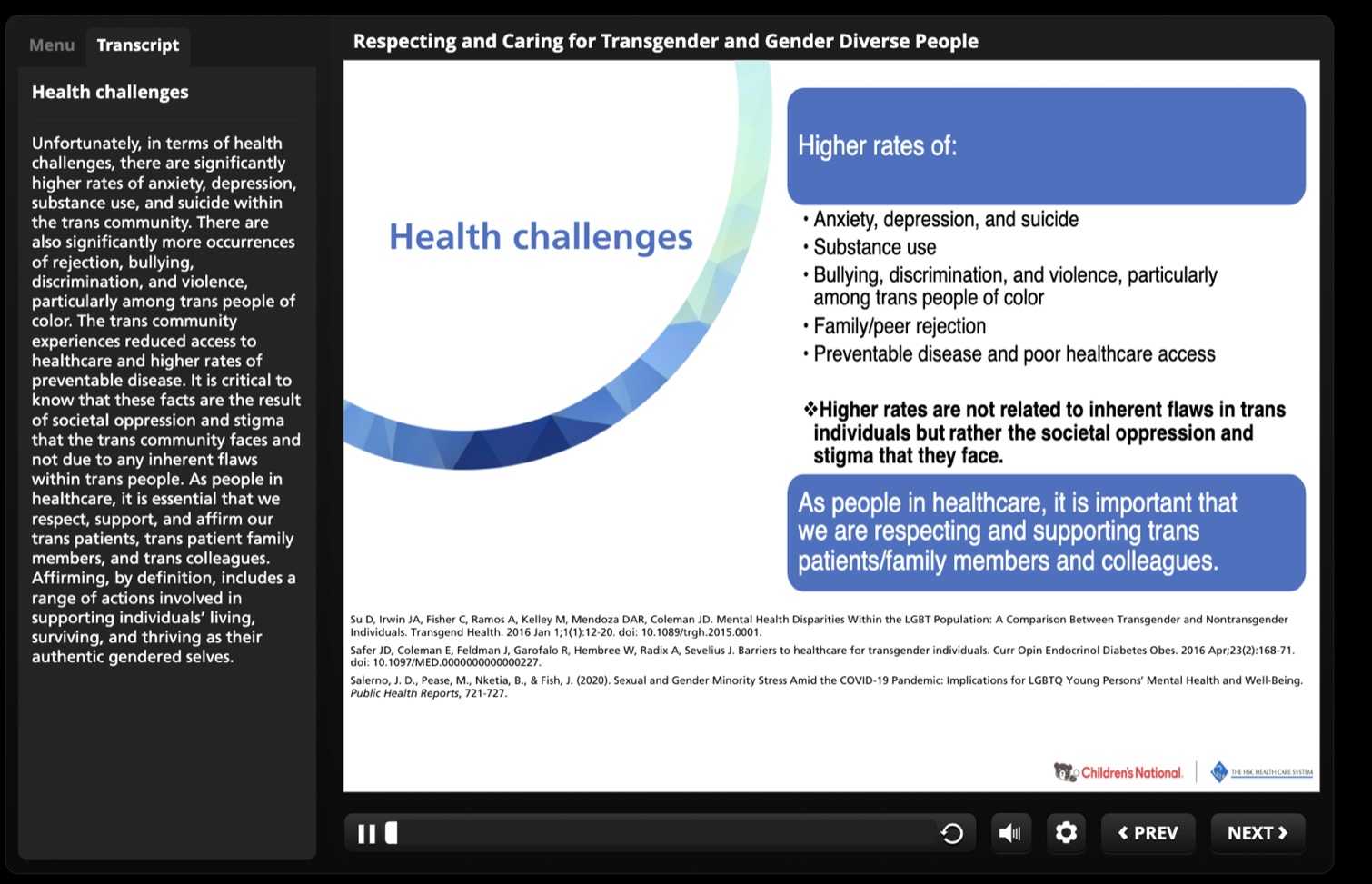
A running theme in the trainings is that transgender people’s high rates of mental illness are due solely to a lack of acceptance. This view, known as the minority stress theory, underpins many of the arguments in favor of on-demand gender affirmation. The training at Children’s National went so far as to suggest that using patients’ preferred pronouns reduces their risk of suicide, echoing the idea that social transition can be “lifesaving.”
There is little evidence to support that claim, said Leor Sapir, a fellow at the Manhattan Institute who studies transgender issues. And by blaming all mental health problems on oppression, the minority stress theory discourages doctors from investigating the root cause of anxiety or depression—or, for that matter, of gender dysphoria.
“It is plausible that many youth with mental health problems are nowadays using ‘born in the wrong body’ as a way to make sense of their [underlying] mental health issues,” Sapir wrote in an email. “Children’s National is very likely making a correlation/causation fallacy.”
The hospital declined to answer specific questions about its training, stating only that it approached gender care “with the utmost seriousness and consideration.” That care, it added, is “consistent” with the standards of the American Academy of Pediatrics, which recommends puberty blockers for children as young as nine.
The Human Rights Campaign did not respond to a request for comment.
The index’s power has been turbocharged by the legal uncertainty around transgender issues, which derives in large part from the policy ping pong between Democrat and Republican administrations. Though former president Donald Trump undid most of the Obama-era rules on LGBT care, the Biden administration has resurrected them and then some—attempting, among other things, to force Catholic hospitals to provide gender-reassignment surgery. With no clear answer about what the law requires, the safest place to be is on the side of the civil rights crusade.
“Lawyers will always advise hospitals to take the most legally defensive course of action,” Sapir said. “In practice, that means deferring to the network of civil rights groups that will sue them.”
It may also mean that nurses like Rempe—who said her objections to gender affirmation were religious as well as clinical—will see their medical conscience rights whither away in the face of activist pressure. In a press release announcing the 2018 edition of the Healthcare Equality Index, the Human Rights Campaign slammed a Trump administration rule that let health workers opt out of facilitating sex changes.
“The measure will directly harm LGBTQ people,” the group said, “by prioritizing physicians’ beliefs over life-saving patient care.”
Hospitals like Children’s National were on notice: provide religious conscience exemptions at your own risk.
“If the index is encouraging things people of faith object to,” said Justin Butterfield, the deputy general counsel of the religious freedom group First Liberty Institute, “then sooner or later it will encourage hospitals to diminish protections for religious employees.”
Now some Republican legislatures are seeking to strike back against the gender juggernaut. Missouri, Florida, Tennessee, Utah, and West Virginia are just some of the red states that have banned puberty blockers, cross-sex hormones, and gender surgeries for minors—measures that could force hospitals in those states to choose between violating the law or accepting a lower Healthcare Equality score.
Hospitals hoping to avoid that choice have a strong incentive to get involved in the legislative fight over gender-affirming care, Morrison said.
Especially since political activism is one of the practices the index rewards.
Hospitals receive points for “community engagement,” the scoring criteria state, if they have “publicly supported LGBTQ+ equality under the law through taking action on local, state, or federal legislation or regulations.”
* Article From: The Washington Free Beacon


